


Case Interpretation | Successful Opening of Acute Right Coronary Artery (RCA) Occlusion with Calcification Using Alveo HP Φ0.75 mm Balloon
Release time:
2024-11-27
For acute occlusion with calcification in right coronary artery (RCA), neither PCI microcatheter nor 1.2/1.0 mm balloons can cross the lesion in emergency treatment??? What other device can be considered by operator in elective operation?
Introduction to the Case
For acute occlusion with calcification in right coronary artery (RCA), neither PCI microcatheter nor 1.2/1.0 mm balloons can cross the lesion in emergency treatment??? What other device can be considered by operator in elective operation?
A Φ0.75 mm Alveo high-pressure balloon is the key to confronting CTO lesion! Let’s dive into this case interpretation.
Recently, a 63-year-old male patient with moderate to high-risk NSTE-ACS underwent his second PCI procedure at a hospital in Xi’an. During the procedure, the operator used a Φ0.75 mm Alveo high-pressure balloon to successfully cross the severe stenosis with calcified lesion in RCA. The balloon was dilated in a single attempt and the stent was implanted successfully! As known, in this case, when the patient was undergoing emergency PCI procedure for the first time, the operator used other brands of balloons and microcatheters, but none of them passed through the severe stenosis with calcified lesion, underscoring the unique advantages of the Alveo HP balloon in clinical applications.
Case information
Patient information: Male, 63 years old, 70 kg
Chief complaint: Intermittent chest tightness and shortness of breath for 12 years, with sudden aggravation for 3 hours.
History of present illness: The patient developed chest tightness and shortness of breath 12 years ago, lasting from a few to tens of minutes, which could be gradually relieved after resting; 3 hours ago during the night rest, the patient experienced sudden chest tightness and shortness of breath that persisted without relief. The patient took nitroglycerin but the symptom was not obviously relieved. After that the patient visited the hospital for treatment.
Past medical history: None
Personal history: 40 years of smoking history, 20 cigarettes/day; 40 years of drinking history, 200 mL/day.
Admission examination
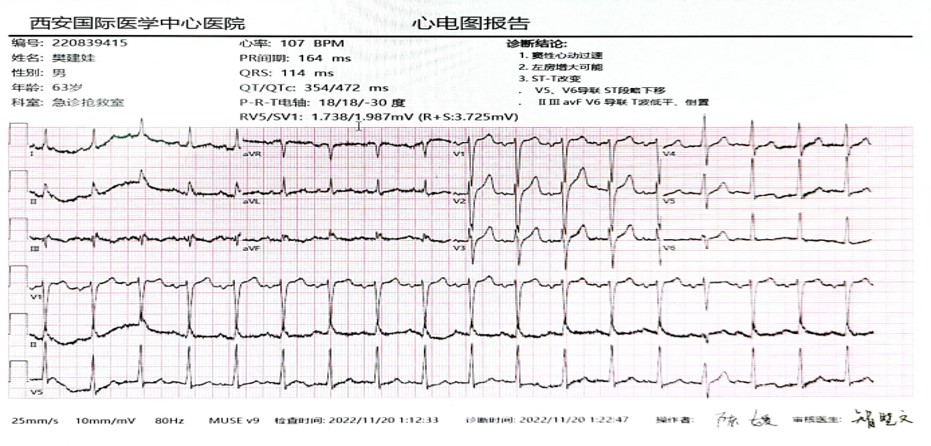
PE: Respiration rate 18 bpm, blood pressure 160/96 mmHG, heart rate 105 bpm, regular rhythm without obvious murmurs auscultated in each valve.
Laboratory tests: The cardiac biomarker panel for myocardial injury were negative, and no obvious abnormality was observed in liver and kidney function electrolytes.
ECG:
Admission treatment: The patient’s symptoms persisted without relief after admission. Dual antiplatelet therapy at a loading dose was given, and the emergency coronary angiography was planned to clarify the coronary artery condition.
Diagnosis result: Preliminary diagnosis of acute coronary syndrome
Pre-operative medication:
Aspirin 300 mg, immediately
Ticagrelor 180 mg, immediately
Atorvastatin calcium tablets, 20 mg, 1 time/night
Metoprolol succinate tablets, 23.75 mg, 1 qd
Coronary angiography
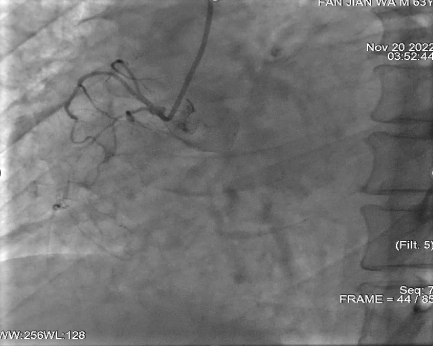
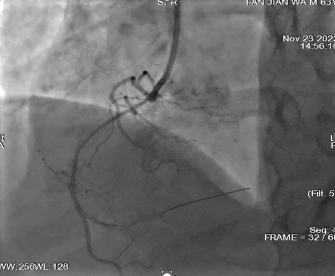
Right coronary angiography: Right coronary occlusion
Left coronary angiography: The circumflex artery retrogradely fills the right coronary artery up to the level of the posterior bifurcation

Left coronary angiography: The anterior descending artery retrogradely fills the right coronary artery up to the level of the posterior bifurcation

Surgical procedure 1
With JR4.0 Guiding, XT-A wire advanced smoothly to the distal end. The microcatheter could not pass through the lesion at the middle segment. The 1.0*15 mm Firefighter balloon was unable to cross the lesion at the middle segment after repeated attempts.
When SAL.75 guiding catheter was used, XT-A wire advanced smoothly to the distal end. The 1.0*15mm Firefighter balloon still could not pass through the lesion at the middle segment after repeated attempts. The guiding catheter displaced from the coronary ostium multiple times during the procedure.
Difficulty Analysis & Surgical Strategy:
The microcatheter and balloon failed to pass through the severe stenosis with calcified lesion after repeated attempts. The angiography revealed that the grade of blood flow at distal segment was TIMI1. The patient’s chest tightness was improved, and the procedure was finished. The Φ0.75 mm Alveo HP Balloon of BrosMed Medical was considered to be used in elective operation later.
Surgical procedure 2
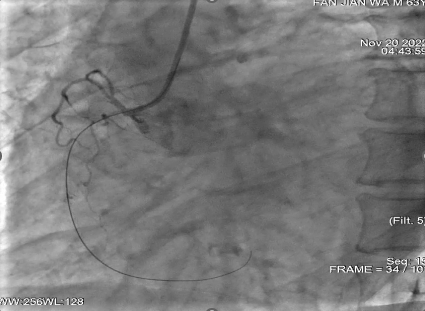
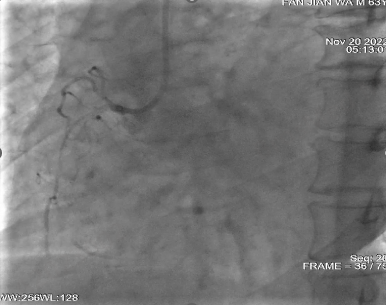
AL.75 Strong Support Guiding Catheter was selected. The Sion guidewire successfully passed through the lesion to the distal end. At this time, a Φ0.75 mm Alveo HP balloon was used to successfully pass through the stenosis with calcification and dilate the lesion from the distal end to the proximal end under a pressure of 16 atm, and then angiography was performed immediately.
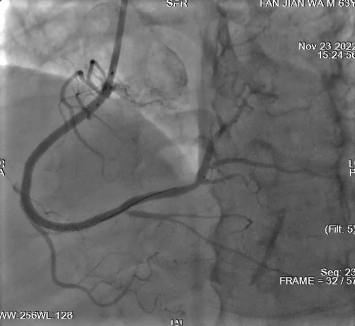
Three stents of 2.5*38 mm, 2.75*38 mm, and 3.0*32 mm were implanted, followed by post-dilation.
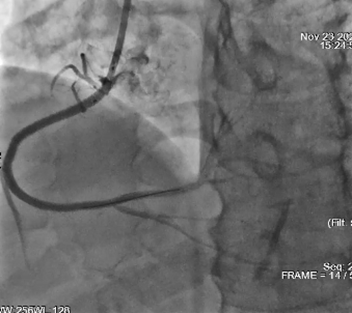 Performing angiography immediately after operation
Performing angiography immediately after operation
Preoperative summary
Assessment of preoperative points
Retrograde flow of both LAD and LCX to RCA, suggesting acute occlusion on the basis of severe stenosis, possibly with presence of intimal calcification or calcified nodules at the lesion site.
Surgical points
After confirming that the guidewire was entered into the true lumen, if none of the microcatheter, 1.0 mm balloon and 1.2 mm balloons could pass through, a stronger support guiding catheter was considered and a smaller-diameter balloon with better passability became the only choice.
Device use points
For patients with long-term smoking history and intimal calcified lesions, whether the balloon can pass smoothly is the basis and prerequisite for subsequent treatment. Alveo HP balloon, as the world’s smallest CTO balloon (with an outer diameter of only Φ0.75 mm), addresses the limitations of conventional balloons and microcatheters in crossing CTO lesions. It is featured by high-pressure tolerance, and a rated burst pressure up to 20ATM. It also offers excellent crossability, withdrawal performance, pushability, and maneuverability. It serves as an essential tool for both emergency and elective PCI, enhancing the success rate of the procedure.
Clinical Cases

The treatment strategy of left main bifurcation lesions has been a controversial topic in clinic. How to choose the optimal treatment strategy for emergency PCI? Does the choice among different devices help the surgeon more?
2024-11-27

Vascular access is the lifeline for hemodialysis patients. Prolonging the service life of the access, guarding the “lifeline” of hemodialysis and ensuring the smooth flow of the “lifeline” are the top priority in maintaining the vascular access. The emergence of the scoring balloon brings the hope of improving patients’ dialysis access patency rate and reducing pain, and is expected to become a better choice for the treatment of arteriovenous fistula stenosis……
2024-11-27
The common symptoms of severe lower limb calcification include coldness, numbness and intermittent claudication in the lower limbs. In severe cases, there may be persistent pain and weakening or disappearance of dorsal foot artery pulsation, and gangrene may occur when the artery is completely occlusive. Calcified lesions destroy the normal blood vessel wall, causing uneven pressure on the blood vessel wall, thinning of some walls, and changes in hemodynamics, which can easily lead to fixed stenosis, thrombus, aneurysm, and aortic dissection.
2024-11-27
 of AVF")
Case Interpretation| Application of Tri-Wedge™ in Juxta-anastomotic Stenosis(JAS) of AVF
In the previous issue of case sharing, we presented a complex coronary intervention case, in which the Alveo HP Φ0.75 balloon, independently developed by BrosMed Medical, demonstrated excellent performance in crossing the lesion and dilation, showcasing exquisite craftsmanship of innovation.
2024-11-27
 Occlusion with Calcification Using Alveo HP Φ0.75 mm Balloon")
For acute occlusion with calcification in right coronary artery (RCA), neither PCI microcatheter nor 1.2/1.0 mm balloons can cross the lesion in emergency treatment??? What other device can be considered by operator in elective operation?
2024-11-27