


Case interpretation | Strategies and examples of endovascular treatment for severe calcification of lower limbs
Release time:
2024-11-27
The common symptoms of severe lower limb calcification include coldness, numbness and intermittent claudication in the lower limbs. In severe cases, there may be persistent pain and weakening or disappearance of dorsal foot artery pulsation, and gangrene may occur when the artery is completely occlusive. Calcified lesions destroy the normal blood vessel wall, causing uneven pressure on the blood vessel wall, thinning of some walls, and changes in hemodynamics, which can easily lead to fixed stenosis, thrombus, aneurysm, and aortic dissection.
Introduction
The common symptoms of severe lower limb calcification include coldness, numbness and intermittent claudication in the lower limbs. In severe cases, there may be persistent pain and weakening or disappearance of dorsal foot artery pulsation, and gangrene may occur when the artery is completely occlusive. Calcified lesions destroy the normal blood vessel wall, causing uneven pressure on the blood vessel wall, thinning of some walls, and changes in hemodynamics, which can easily lead to fixed stenosis, thrombus, aneurysm, and aortic dissection.
Two methods are commonly used for calcification typing. The first method uses CTA, DSA and IVUS to evaluate the calcification degree at the lesion site; the second method uses the Peripheral Artery Calcification Scoring System (PACSS).
Both analysis systems divide the calcification degree into four grades. The first method divides the blood vessel cross-section into four quadrants, and uses the number of quadrants occupied by calcified lesions to indicate the severity grade. The second method, combined with high-intensity fluoroscopy and DSA imaging, classifies the calcification degree of target lesions into grades 0 to 4.
Treatment strategies for the calcified lesions include lumen expansion and plaque removal, and treatment methods vary depending on the lesion site. For iliac artery lesions, stent implantation is preferred; for common femoral artery lesions, plaque removal and blood vessel dredging are preferred clinically, without leaving any graft; for severe calcified lesions in the short segment of the superficial femoral artery, volume reduction plus drug-coated balloon therapy is clinically preferred.
In this case, we will have a detailed understanding of the specific surgical strategies and procedures for severe calcified lesions below the knee.
Patient Profile
Patient information: Male, 70 years old, 75 kg
Visiting time: 10/9/2023
Chief complaint: coldness and pain in both lower limbs for 7 years, aggravation with intermittent ulceration for 4 years
Present illness: The patient reported chills in both lower limbs 7 years ago, accompanied by intermittent claudication with a claudication distance of about 200 meters. He underwent balloon dilatation plasty in a tertiary hospital in Beijing, but the postoperative relief was not obvious. In the past 4 years, he had intermittently suffered from toe ulcerations, accompanied by exudation and pus, and was treated in several tertiary hospitals in Beijing. After multiple interventions and treatment with negative pressure sealing and drainage, the wound was close to healing. The patient was admitted to hospital for aggravated intermittent claudication with rest pain.
Past history: Hypertension, type 2 diabetes, coronary heart disease, old cerebral infarction, reflux esophagitis.
Risk factors: Type 2 diabetes
Admission examination
Physical examination: No obvious abnormalities were found in general physical examination. Weak pulse of femoral artery and popliteal artery in both lower limbs. The bilateral dorsalis pedis and posterior tibial arteries were not palpable.
Laboratory tests: Hemoglobin 151g/L, albumin 46.4g/L, creatinine 78μmol/L, Ca 2.39mmol/L, P 1.02mmol/L, K 4.01mmol/L, CO2 25.9mmol/L
Diagnosis: Atherosclerosis obliterans of lower limbs
Preoperative Examination
Lower Limb Artery CTA:
· Severe stenosis in the proximal segment of the right internal iliac artery;
· Luminal occlusion in the bilateral posterior tibial arteries and the left anterior tibial artery;
· In-stent lumen occlusion in the proximal segment of the right posterior tibial artery and distal segment of the left anterior tibial artery
Preoperative discussion
- The patient’s lower limb artery CTA indicated that there were severe stenosis or even occlusion of blood vessels in many places, and conservative treatment could not effectively improve the patient’s symptoms. Interventional surgery was considered to open the occluded blood vessels in the patient’s lower limbs and promote wound healing.
- Combined with the patient’s symptoms, signs and examination results, the arteriography, laser ablation and balloon dilatation were planned to perform on the right lower limb.
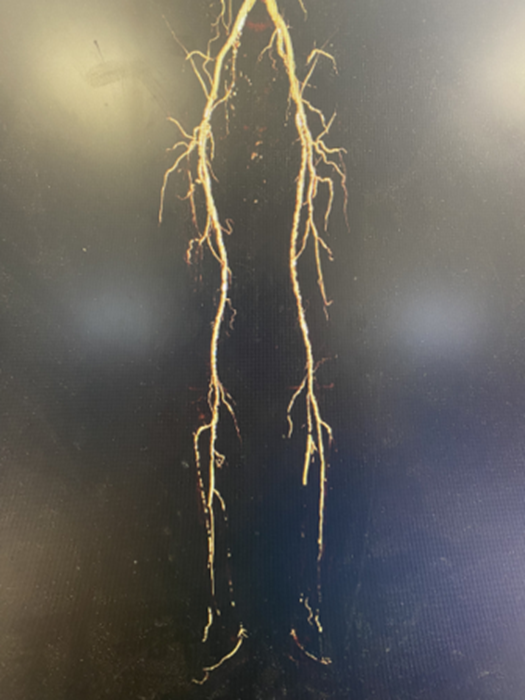
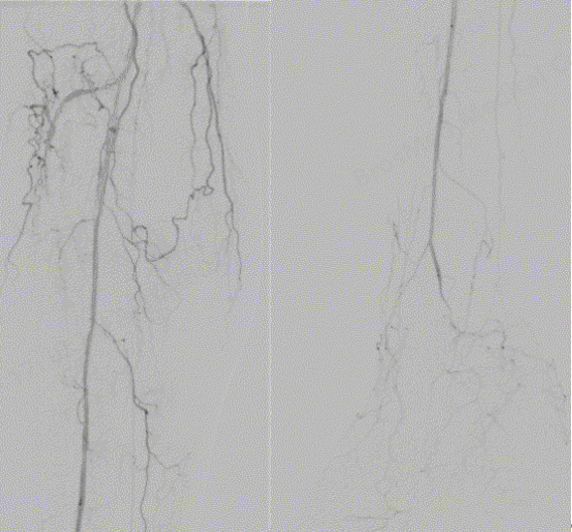
Preoperative Angiography
 Small lumen of the tibiofibular trunk
Small lumen of the tibiofibular trunk
 Anterior tibial and posterior tibial arteries not visualized
Anterior tibial and posterior tibial arteries not visualized
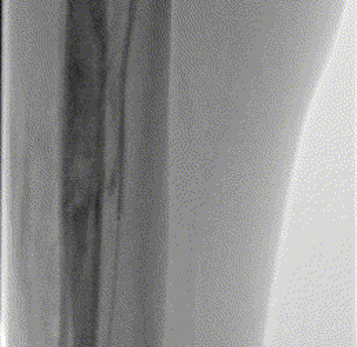
 Proximal occlusion of the peroneal artery with localized distal luminal narrowing
Proximal occlusion of the peroneal artery with localized distal luminal narrowing
Angiographic analysis:
PAD revascularization needed
Primary objective:
To open the tibiofibular trunk and peroneal arteries
Surgical Procedure
Turbo-Elite laser atherectomy catheter opened the tibiofibular trunk and peroneal arteries
BrosMed Tri-Wedge™ PTA scoring balloon dilation catheter (3.0mm×60mm) was used to dilate the tibiofibular trunk and to open the peroneal artery ostium. First, inflation at 4 atm for 10s, then increase to 6 atm, and the lesion was opened.
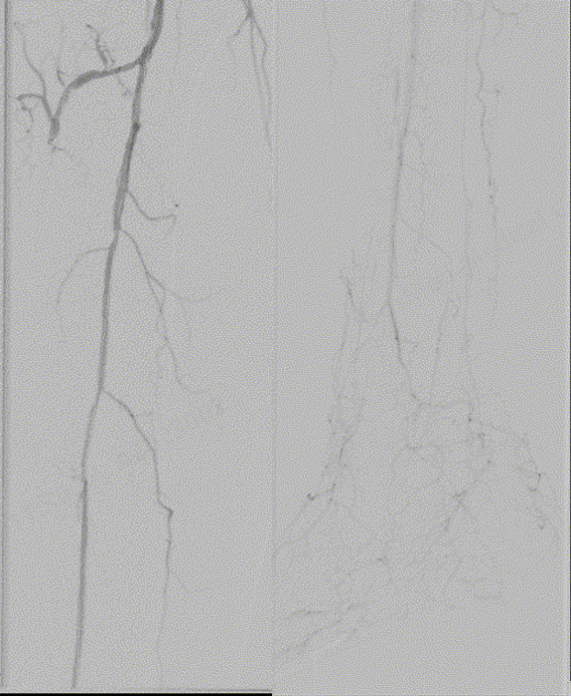
Post-dilation angiography showed patency of the tibiofibular trunk and peroneal artery
BrosMed Bachilles PTA balloon catheter (2.5mm × 150mm) was used for further dilatation
Post-dilation angiography showed patency of target lesion and the flow rate was satisfactory.
DCB was adopted for further dilatation
Post-dilation angiography showed patency of target lesion and the flow rate was satisfactory.
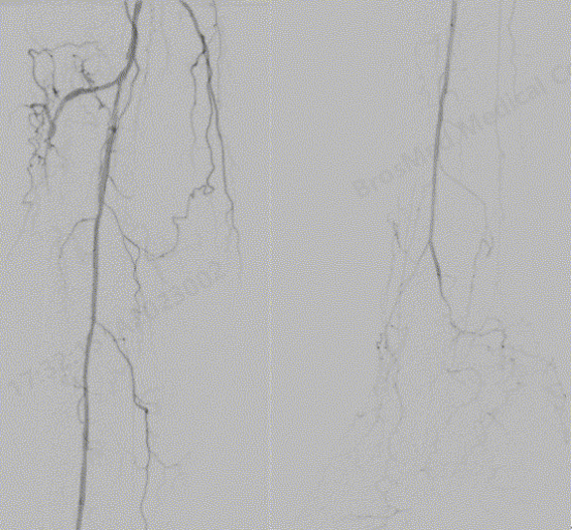
Postoperative Comparison
 Preoperative image
Preoperative image
 Preoperative image
Preoperative image
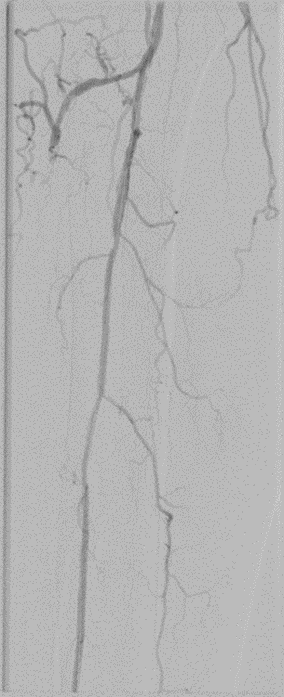 Postoperative image
Postoperative image
Summary
The patient’s intraoperative angiography showed the superficial femoral artery and popliteal artery lumen were unobstructed, and the main lesions were in the infrapopliteal artery, including severe stenosis of tibiofibular trunk, occlusion of proximal peroneal artery, with outflow tract seen at distal end; occlusion of anterior tibial artery and posterior tibial artery, without outflow tract seen at the distal end.
During the operation, a laser catheter was first used to open the lumen. Considering the severe lesions at the tibiofibular trunk and the proximal end of the peroneal artery, the ordinary balloon dilation was not effective. The BrosMed Tri-Wedge™ scoring balloon 3.0mm×60mm dilation catheter was used for dilation, and angiography showed that the lumen was unobstructed and the flow rate was slow. The occluded segment of the tibiofibular trunk and peroneal artery were dilated with BrosMed Bachilles 2.5mm × 150mm non-compliant PTA balloon catheter and drug-coated balloon catheter, and the post-dilation angiography showed that the lumen was unobstructed and the flow rate was satisfactory.
Case Summary
01
Case characteristics: The patient’s main symptoms were coldness and pain in the lower limbs accompanied by ulceration of the right foot. Physical examination indicated weak pulses of the femoral artery and popliteal artery of both lower limbs; the bilateral dorsalis pedis and posterior tibial arteries were not palpable.
02
Key points of preoperative evaluation: Physical examination and imaging evaluation showed that the patient’s right below-the-knee artery was severely occluded and the right foot was ulcerated. The main purpose was to open the right below-the-knee artery and promote wound healing.
03
Key points of operation: The superficial femoral artery was punctured anteriorly, a wire guide catheter was inserted into the distal end of peroneal artery, and a 3.0mm×60mm peripheral vascular scoring balloon dilation catheter was selected.Tri-Wedge™ scoring balloon was accurately delivered to the tibiofibular trunk and peroneal artery under CT guidance, and then slowly inflated for dilatation.
Post-operation angiography showed patency of target lesion and the flow rate was satisfactory. After withdrawing the balloon catheter, angiography showed that the lumen at the tibiofibular trunk and the opening of peroneal artery was unobstructed and the flow rate was satisfactory.
04
Key points for using the Tri-Wedge™ scoring balloon:
- The balloon dilates the high-resistance lesion sites and prolong the re-occlusion time of the arterial lumen
- Designed with special balloon material and super-smooth hydrophilic coating, it improves overall compliance and tracking, and can easily pass through tortuous and narrow lesions.
- The balloon is gradually inflated by pressure, enabling the scoring wires to exert the collected pressure on the vessel wall, which improves the success rate of the operation while reducing the expansion pressure
Clinical Cases

The treatment strategy of left main bifurcation lesions has been a controversial topic in clinic. How to choose the optimal treatment strategy for emergency PCI? Does the choice among different devices help the surgeon more?
2024-11-27

Vascular access is the lifeline for hemodialysis patients. Prolonging the service life of the access, guarding the “lifeline” of hemodialysis and ensuring the smooth flow of the “lifeline” are the top priority in maintaining the vascular access. The emergence of the scoring balloon brings the hope of improving patients’ dialysis access patency rate and reducing pain, and is expected to become a better choice for the treatment of arteriovenous fistula stenosis……
2024-11-27
The common symptoms of severe lower limb calcification include coldness, numbness and intermittent claudication in the lower limbs. In severe cases, there may be persistent pain and weakening or disappearance of dorsal foot artery pulsation, and gangrene may occur when the artery is completely occlusive. Calcified lesions destroy the normal blood vessel wall, causing uneven pressure on the blood vessel wall, thinning of some walls, and changes in hemodynamics, which can easily lead to fixed stenosis, thrombus, aneurysm, and aortic dissection.
2024-11-27
 of AVF")
Case Interpretation| Application of Tri-Wedge™ in Juxta-anastomotic Stenosis(JAS) of AVF
In the previous issue of case sharing, we presented a complex coronary intervention case, in which the Alveo HP Φ0.75 balloon, independently developed by BrosMed Medical, demonstrated excellent performance in crossing the lesion and dilation, showcasing exquisite craftsmanship of innovation.
2024-11-27
 Occlusion with Calcification Using Alveo HP Φ0.75 mm Balloon")
For acute occlusion with calcification in right coronary artery (RCA), neither PCI microcatheter nor 1.2/1.0 mm balloons can cross the lesion in emergency treatment??? What other device can be considered by operator in elective operation?
2024-11-27